
For the spay-neuter vet, pandemic social distancing has been a slow time. I’ve had plenty of opportunity to stay home sleeping, baking, playing Pokemon Go and watching birds (often these two are simultaneous activities), eating fiddleheads, and seeing spring unfurl. With services starting to reopen, I’m getting ready to go back to work on Monday, so my thoughts have started to turn back to surgery and ergonomics.
During these idle months I’ve had some time to look through old ergonomics articles and projects with an eye to assembling them into something useful. This week I found myself thinking about needle holder grasps (after a Facebook conversation) and thought to look back at my masters thesis in ergonomics. The topic was a comparison between palm grasp and tripod (fingers in the rings) grasp for needle holders. The aim was to compare users of the two techniques both by surveying them about pain and by measuring the muscular strain in their forearms. In keeping with my desire to share incidental and independent research results, I’m publishing the thesis at the bottom of this blog post (never fear, we were limited to 5000 words).
If you thought this article would answer the question of whether palm grasp is better than placing fingers in the rings of the instrument, think again! The utter messiness of the results and the difficulty of drawing conclusions about the different grasp types was why I never published it anywhere (until now! here!). But I learned a lot from the research about individual variability and the diversity of supposedly standardized techniques. This paragraph taken from the Discussion sums up what I learned:
The amount of grasp diversity between participants, the use of non-standard instrument grasps, and the variability in individual participants’ grasps, were surprising findings in the current study. Participants were often unaware of the grasp that they used. Several described themselves using a grasp different from the one that they actually used, and some noticed in the midst of the experiment that they were using a different grasp from what they had described. Even within a single grasp type, the participants varied in their movement patterns and degrees of forearm rotation and wrist angulation.
So while I can’t promise any groundbreaking information about which grasp style is ergonomically superior, I do think there are some interesting photos and tidbits in this article. I also think that the diversity of successful techniques leaves clear opportunity for individuals to modify their grasping and suturing technique if and when it becomes painful or problematic for them.
I hope you all are well, and staying safe. Enjoy!
Electromyographic analysis of needle-holder grasps used while suturing
A thesis in partial fulfillment of Masters of Science in Health Ergonomics, University of Derby, February, 2015
Abstract
The current study examined variations in muscular force and muscle use patterns between surgeons using different grasps while suturing. Fourteen (4 male, 10 female) right-handed veterinarians were recruited into one of two groups, palm or tripod, depending on their usual, preferred needle holder grasp. Participants completed the Cornell Musculoskeletal Discomfort Questionnaire (CMDQ) and the Cornell Hand Discomfort Questionnaire (CHDQ), and then performed a suturing task using their preferred grasp. Four muscles in the right forearm region were selected for electromyographic (EMG) recording: extensor digitorum communis (EDC), flexor carpi radialis (FCR), flexor carpi ulnaris (FCU) and abductor pollicis longus/ extensor pollicis brevis (APL).
The 1-week period prevalence of MSD was 92.9%, with 13 of 14 participants reporting pain. Of these, 7 (50%) reported hand pain, and 12 (85.7%) reported body pain. Observed grasps differed from those reported by participants, with five using exclusively tripod grasp with the thumb and ring finger in the instrument rings, two using a modified tripod grasp with thumb and middle finger, three using palm grasp for suture placement and tripod grasp during needle extraction and knot tying, three using palm grasp with no fingers in the instrument rings, and one using palm grasp with the ring finger in one instrument ring. The static load (10th% APDF) on each of the four muscles ranged from 0.9 to 10% MVC, with greater mean values for the extensor EDC than for the flexors FCR and FCU. Degrees of forearm pronation and supination ranged from 80 to 180 degrees, and degree of rotation was positively correlated with the total pain score. Future investigation into the characteristics and benefits of various grasps is warranted, so that practical advice on reducing strain and MSD risk can be offered to surgeons.
Introduction
High-volume spay-neuter is a growing practice area in veterinary medicine in the US (Looney et al., 2008) in which veterinarians may perform over 30 surgical procedures daily, and some individuals spend over 35 hours each week performing surgery (White, 2013). These procedures are of limited variety compared with general surgery, and frequently involve static postures and repetitive manual tasks. Repetitive work is associated with increases in upper limb discomfort, tendinitis, and carpal tunnel syndrome in people who engage in manual work (Latko et al., 1999), and static postures, or isometric positions where little movement takes place, multiply the risk for musculoskeletal disorders attributable to those postures (Esser et al., 2007). While work in high volume spay-neuter has many qualities that would appear to put veterinarians at risk for MSD, there is limited research on the effects of this repetitive surgical workload on veterinarians, and no research exploring ways to mitigate these effects.
A single cross-sectional study (White, 2013) has investigated musculoskeletal discomfort (MSD) in veterinarians working in high-volume spay-neuter. The one-month period prevalence of MSD was 99.1%, with 76.7% experiencing hand or wrist pain and 98.2% experiencing body pain. Hand discomfort was most commonly reported in the right thumb and/or thumb base (49.8%) and the right wrist (37.9%). This rate of hand/wrist discomfort is 1.5 to 2 times the prevalence of upper limb MSD experienced by veterinarians in general practice (Kozak et al., 2014; Scuffham et al., 2010; Smith et al., 2009), and greater than the prevalence in surgeons in human surgical practice (Adams et al., 2013; Soueid et al., 2010). Body discomfort in spay-neuter veterinarians was most commonly reported in the lower back (76.7%), shoulders (72.6%), and neck (71.7%). Three-quarters of veterinarians experiencing hand, finger, and thumb MSD attributed their MSD completely to their work in spay-neuter. Increasing career length, increasing weekly hours in surgery and decreasing job satisfaction were the work-related factors with the greatest relative contribution accounting for variation in hand pain severity and total pain. While 94.4% of respondents felt that posture and positioning during surgery is important, only 30.6% had received any instruction in posture, positioning, or ergonomics in surgery (White, 2013).
The high prevalence of upper limb MSD in spay-neuter veterinarians may be related to the high volume and limited variety of surgical tasks undertaken, and thus the repetition of a limited diversity of hand movement patterns performed in the workday. Anecdotally, some spay-neuter veterinarians have attributed their lack of upper limb MSD to their use of a palm grasp when using needle holders, instead placing their fingers in the instrument rings.
Textbooks and authors vary in their use of terms to describe instrument grip. Anderson and Romfh (1980) describe the “palmed grip” in which the surgeon grips a long needle holder by the shanks, away from the finger rings and ratchet, making it impossible to open or close the ratchet while using this grip. This is in contrast to Seki’s (1988) diagram of “grip 2,” in which the finger rings and ratchet are held in the palm of the hand, allowing operation of the ratchet mechanism. This is the same as the “modified thenar eminence grip” described by Toombs and Bauer (1993), and also described (though unnamed), two decades earlier (Weiss, 1973). More recent sources (Kirpensteijn & Klein, 2006; Yoon & Mann, 2011) name this same grasp the “palm grip.” Yoon and Mann (2011) use the term “thenar eminence grip” to describe a grasp in which the needle holder is grasped in the palm, with the tip of the ring finger placed through one finger ring. The same grasp is elsewhere called the “thenar grip” (Anderson & Romfh, 1980). Booth (2013) repeats the descriptions and terms used by Anderson and Romfh (1980), except that, in the illustration of Booth’s “thenar grip,” the fourth finger does not enter the finger ring, making this “thenar grip” resemble the “palm grip” described above.
Current consensus appears to favor “palm grip” to describe the grasp in which the finger rings and ratchet are held in the palm, with no fingers in the finger rings. The comparison grip, utilizing thumb and ring finger in the instrument rings, has been called the three point grip (Kirpensteijn & Klein, 2006), the thumb-ring finger grip (Anderson & Romfh, 1980), the thumb-third finger grip (Toombs & Bauer, 1993) [this grip is pictured with the fourth phalanx in the instrument ring, despite the use of “third finger” in the name], and thumb-ring finger (tripod) grip (Booth, 2013). For the current study, the term “tripod grip” has been chosen for its brevity and clarity.
The research comparing the attributes, physics, and precision of these grasps during open (non-laparoscopic) surgery is limited. One study found greater suturing precision among surgeons using palm grasp as compared to tripod grasp (Seki, 1988), and the author speculated that the palm grasp was more stable and reduced the difference in angle between the hand and the instrument. Despite the limited research comparing the grasps, surgical textbooks make assertions about their qualities and disadvantages. Toombs and Bauer (1993) state that the modified thenar eminence (palm) grip results in imprecise release of the needle, making this grip poorly suited to delicate suturing compared to the thumb-third finger (tripod) grip. This contrasts with Seki’s (1988) finding of greater accuracy when using the palm grip.
Several studies have used electromyography (EMG) to compare the ergonomic aspects of various grasps. Surface EMG uses electrodes on the skin to detect the electrical activity produced by the summed motor unit action potentials in the muscle of interest (Criswell, 2011). EMG signal strength has an approximately linear relationship with muscular force, making it useful in ergonomics for determining the amount of individual muscle involvement in a given task, and allowing evaluation of strain on the tissues (Hägg et al., 2004). One study comparing two different grasp styles on a laparoscopic instrument found differences in EMG amplitude in several forearm muscle groups, leading to the recommendation of a specific, palm-grasp style in certain circumstances (Berguer et al., 1999). A second study comparing various laparoscopic handle designs found that the pattern of EMG activity—the proportional use of each measured muscle—is characteristic of the handle (and thus the grasp) used, rather than being task-specific (Matern et al., 2004). A similar EMG study of handwriting grasp styles also showed characteristic EMG activation patterns for each grasp style (de Almeida et al., 2013).
The amplitude probability distribution function (APDF) is a means of EMG data reduction that is used to characterize the muscular load profile over a period of time (Hägg et al., 2004). The calculation reveals the cumulative probability for EMG amplitude over time, and can be normalized for each subject to a percentage of their maximum voluntary contraction (%MVC) for that muscle. APDF levels are often reported as 10th, 50th, and 90th percentiles, with 10th %APDF representing static load, 50th% APDF median load, and 90th% APDF considered peak load for that muscle (Szeto et al., 2009).
The current study aimed to examine variations in muscular force and muscle use patterns between surgeons using a palm grasp versus a tripod grasp while suturing. It was expected that the results could be used to guide surgeons in selecting which grasp to use routinely, and indicate which grasp to choose or avoid to decrease strain on specific muscles and their associated tendons and ligaments.
Methods
Participants
A total of 14 (4 male, 10 female) veterinarians were recruited for the present study. Participants were recruited into one of two groups, palm or tripod, depending on their usual, preferred needle holder grasp pattern. All subjects were right-handed.
Participants were recruited at two veterinary conferences: the North American Spay/Neuter Conference in Austin, Texas and the Silicon Valley Spay & Neuter Symposium in Milpitas, California, in 2014. Two additional veterinarians were recruited at a spay/neuter strategy meeting in Burlington, Vermont. Consent to participate was obtained from each participant before the study began. The study was approved by the Psychology Research Ethics Committee at the University of Derby
All participants in the study were asked to complete a questionnaire prior to participation. Demographic data including year of birth, year of graduation from veterinary school, whether they have obtained any specialty certification, and current hours per week performing surgery were recorded. Participants were shown pictures of “palm” and “tripod” grasps, and asked which grasp they use, or, if a mixture of grasps, in what proportion they use those grasps. They were also asked when they began using their current instrument grasp, whether they have used a different grasp at any point in their career, and why they have chosen their current instrument grasp.
In addition, participants were asked to complete the Cornell Musculoskeletal Discomfort Questionnaire and the Cornell Hand Discomfort Questionnaire regarding any discomfort in the past week. These questionnaires allowed the determination of the location, severity, and impact on work and daily activities.
Electromyography
Four muscles in the right forearm region were selected for the electro- myography (EMG) study: extensor digitorum communis (EDC), flexor carpi radialis (FCR), flexor carpi ulnaris (FCU) and abductor pollicis longus/ extensor pollicis brevis (APL). The I-330-C2+ system (J&J Engineering, Inc., Poulsboro, WA) was used to capture the surface EMG data, with a bandwidth of 10-400 Hz and a common mode rejection ratio of 100 dB, with input impedance 10 GW and a notch filter of 60 Hz. The EMG signals underwent a 16 bit analogue to digital (A/D) conversion at a sampling frequency of 1024 Hz.
Bipolar Ag-AgCl surface electrodes (Norotrode 20, Myotronics, Inc, Kent, WA) with an inter-electrode spacing of 22 mm were used. The ground electrode was an 1 3/8 inch Ag-AgCl electrode (SilveRest, Vermed, Bellows Falls, VT) that was placed on the right upper arm above the elbow.
The locations for EMG electrodes were adopted from Perotto (2011) and Criswell (2011). Before attaching electrodes, the skin was prepared by abrading with a gauze sponge. After electrode placement, the skin impedance was checked using the impedance testing function in the I-330-C2+, and impedance below 900 KW was considered acceptable.
Prior to starting the experiment, subjects were asked to perform two trials of resisted isometric maximum voluntary contractions (MVC) of 5 seconds each against manual resistance for each muscle.
Video Recording
Each session was recorded using 1080p HD video at 30 frames per second using an iPhone 5S (Apple, Inc, Cupertino, CA). A single, front view recording of each participant was made, and markers in the EMG recording allowed synchronization of video and EMG recordings.
Video recordings were used to examine posture during surgery using Rapid Upper Limb Assessment (McAtamney & Corlett, 1993). RULA assessment was made at the time in the work cycle when the highest loads occurred, assessing the participant’s dominant arm, and applied just to the experimental condition (not extrapolated to a “typical” work day).
Protocol
Each participant stood at a table adjusted to their preferred height. Participants were then asked to use an 5.5 inch Olsen-Hegar needle holder (Spectrum Surgical, Stow, OH) and thumb forceps to place five simple interrupted sutures in a polyvinyl alcohol synthetic chamois skin model using 3-0 Monocryl suture on a 40 mm, ½ circle taper needle. Measurements taken during the first suture were not included in the analysis, in order to allow the surgeon to become familiar with the materials and task.
Data Processing and Analysis
The USE3 Physiolab (J&J Engineering, Inc., Poulsboro, WA) software was used to process the EMG data. Data processing involved full-wave rectification and smoothing with root-mean-square (RMS) with a 250 ms window. These data were then exported to Microsoft Excel to compute the MVCs for each muscle, and to SPSS to compute the 10th%, 50th% and 90th% levels of Amplitude Probability Distribution Function (APDF) for the four muscle groups.
Pain severity for each body region was calculated for each participant using the scoring guidelines accompanying the CMDQ and CMHQ (Hedge, n.d.). Frequency scores were assigned: never = 0; 1–2 times a week = 1.5; 3-4 times a week = 3.5; every day = 5; several times a day = 10. Discomfort scores were assigned: slightly uncomfortable = 1; moderately uncomfortable = 2; very uncomfortable = 3. Daily interference scores were assigned: not at all = 1; slightly interfered = 2; substantially interfered = 3. Pain severity was obtained by multiplying the frequency, discomfort, and interference scores for each body part. Total body pain severity for an individual was obtained by summing all the body pain severity scores for that individual. Total hand pain scores were obtained by summing the hand pain severity scores for that individual. Total overall pain scores were obtained by summing the hand pain and body pain scores for that participant.
Demographic, MSD, and EMG data were entered into SPSS. Pearson correlations were used to assess relationships between MSD and demographic and postural characteristics. APDF levels of different muscles were compared using paired sample t-tests.
Results
Demographics
A total of 14 veterinarians participated in this study, including 10 (71.4%) females and 4 (28.6%) males (Table 1). The median age of participants was 43 years, with a range of 31 to 62 years of age. Median time since graduation from veterinary school was 13.5 years, with a range of 4 to 32 years. None of the veterinarians had obtained board specialty certification. Participants spent a median of 17.5 hours a week in surgery, with a range from 0 to 35 hours weekly. Two participants did not regularly perform surgery in their current jobs: one was in a management position and performed surgery on an as-needed basis, and the other was seeking employment. Both of these veterinarians had several years experience performing surgery.

Musculoskeletal Discomfort Prevalence
The self-reported 1-week period prevalence of MSD was 92.9%, with 13 of 14 participants reporting pain. Of these, 7 (50%) reported hand pain, and 12 (85.7%) reported body pain. All who reported discomfort also reported that it interfered at least slightly with their ability to work. In the right hand, the most commonly reported areas of MSD were the distal thumb (first proximal and distal phalangeal area; 28.6%), and the thumb base (first metacarpal area; 28.6%). MSD was reported in some portion of the right thumb [phalangeal and metacarpal areas] by 42.8% of participants. Body MSD was most commonly reported in the lower back (71.4%), right shoulder (50%), and neck (50%).
Pain severity was not correlated with age (r (12)= 0.233, p= 0.424) or hours per week in surgery (r (12)= 0.005, p= 0.987), and was unrelated to the sex of the participant (t(12) = -1.415, p=0.182).
Grasp Characteristics
Eight of the participants reported using tripod grasp all or most of the time, and 5 reported using palm grasp all or most of the time. The remaining surgeon reported using the two grasps equally. Eleven participants (78.6%) reported having adopted their current grasp in veterinary school or before, whereas 3 participants (21.4%) reported to have modified their grasp after graduation from school.
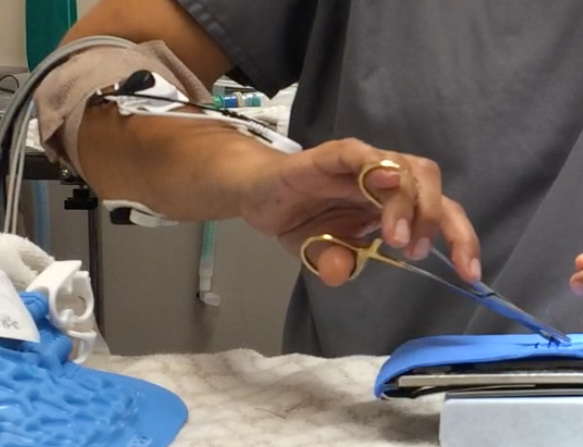
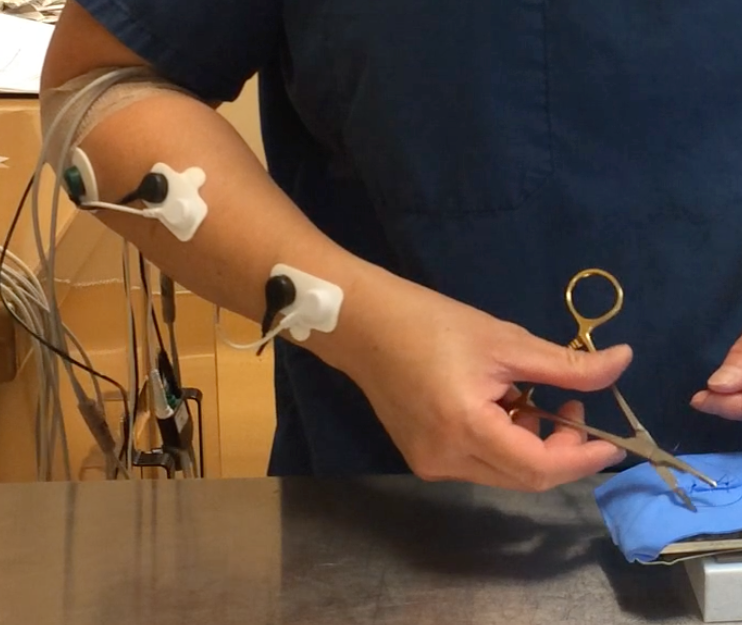
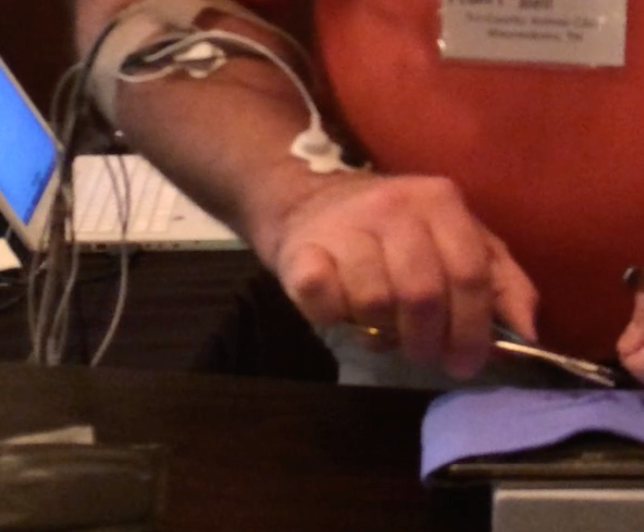
Actual observed grasps differed from those reported by participants (Figures 1-5). Video analysis revealed that 5 participants used exclusively tripod grasp with the thumb and ring finger in the instrument rings (1, 4 tripod), one of whom routinely placed her fifth finger in the instrument ring with her fourth finger. Two participants used a modified tripod grasp with the thumb and middle finger (1, 3 tripod) in the instrument rings. Three participants used palm grip for suture placement (driving the needle through the substrate) and switched to 1, 4 tripod grasp during needle extraction and knot tying (palm/tripod). Three participants used palm grasp with no fingers in the instrument rings, and one participant used a palm grasp with the ring finger in one instrument ring.


Electromyography
Results of electromyographic recordings are presented in Table 2. In one participant, EMG readings were not obtained for FCU activity, as the electrodes loosened during the experiment.

EDC: extensor digitorum communis, FCR: flexor carpi radialis, FCU: flexor carpi ulnaris, APL: abductor pollicis longus/ extensor pollicis brevis.
*FCU electrodes loosened on Participant 7, preventing data collection from this muscle
The 10th % APDF, representing the static load on each of the four muscles, ranged from 0.9 to 10% MVC, with greater mean values for the extensor EDC (M = 5.51; SD = 1.37) than for the flexors FCR (M = 3.27, SD= 1.62) and FCU (M = 3.33, SD=1.53). These differences were statistically significant, with EDC:FCR t(13) = 5.082, p<0.001 and EDC:FCU t(12) = 4.824, p<0.001, two tailed. This differential activation level persisted between the EDC and FCU at the 50th and 90th % APDF, whereas the mean activity level of the FCR increased by the 50th and 90th % APDF so that there was no difference at either time between EDC and FCR activation levels (Figure 6).

EDC: extensor digitorum communis, FCU: flexor carpi ulnaris, FCR: flexor carpi radialis.
* significant difference between mean activation levels.
The unexpected diversity of grasp styles and small number of participants using each grasp prevented adequate comparisons of muscle activation patterns between grasps.
Postural comparisons
RULA assessments produced scores of 3 or 4 in all subjects, indicating that overall postural scores did not differ substantially between subjects, and that all fell into the moderate risk category. Variations in the degrees forearm pronation and supination were noted between subjects, with a range of 80 to 180 degrees of rotation (M= 125, SD = 26.5). The degree of rotation did not appear to be related to the instrument grasp, and was positively correlated with the total pain score determined on the CMDQ and CHDQ questionnaires (r (12)= 0.556, p= 0.039).
Discussion
There has been little previous research into the physical demands of high volume spay neuter surgery. A previous study of MSD prevalence in spay neuter veterinarians (White, 2013) found a 99.1% one-month period prevalence of MSD, which is slightly higher than the 92.9% one-week period prevalence reported in the current study. The body sites with the highest prevalence of MSD were the same in the two studies, with participants most often reporting body MSD in the lower back, shoulders and neck, and hand MSD in the right distal thumb and in the right thumb base. The previous study demonstrated increased MSD risk with increased weekly surgery hours and increased years of work, an effect not seen in the current study. However, these factors had weak explanatory power, accounting for less than 5% of the variability in MSD scores. This small effect size, paired with the smaller sample size in the current study, may account for this lack of effect. Neither study showed an effect of gender on MSD prevalence.
The EMG findings of greater static load on extensors compared to flexors is likely due to the extension of the metacarpophalangeal joints required to execute any of the needle holder grasps. During median and high load conditions, greater need for wrist flexion increases flexor load. Some of the increase with load in the FCR readings may also be due to crosstalk with the superficial digital flexor (Criswell, 2011), and may be related to creating a tighter instrument grasp as greater force is required.
The amount of grasp diversity between participants, the use of non-standard instrument grasps, and the variability in individual participants’ grasps, were surprising findings in the current study. Participants were often unaware of the grasp that they used. Several described themselves using a grasp different from the one that they actually used, and some noticed in the midst of the experiment that they were using a different grasp from what they had described. Even within a single grasp type, the participants varied in their movement patterns and degrees of forearm rotation and wrist angulation.
Most of the participants claimed to have used their current instrument grasp beginning in veterinary school. However, the wide diversity of grasps, and the use of grasps not described in most veterinary or surgical texts, suggests either that the participants modified their grasps after leaving school, or that their veterinary surgical instructors taught or at least tolerated unconventional grasps. It is also possible that participants’ initial surgery instruction in veterinary school taught conventional instrument grasps, but that later in the curriculum, instructors failed to notice or failed to correct unusual grasps.
After leaving veterinary school, few practitioners receive instruction in instrument grasp or the biomechanics of surgical technique. Veterinary continuing education in surgery emphasizes processes at the “sharp” end of the instrument — the interface between instrument and patient tissue — but generally does not address the interaction between surgeon and instrument. Thus, practitioners are typically on their own as they develop and encode the motor sequences that comprise their practice of surgery.
The process of acquisition of a motor skill such as suturing requires initial cognitive attention to the task and its components. After repetition, performance becomes smoother and the need to concentrate on the task decreases. Finally, the motor sequence becomes automated and the skilled performer loses conscious awareness of individual motor actions (Ericsson, 2004). This automation of learned action sequences into performance units occurs slowly through repetition without requiring conscious awareness (Graybiel, 1998).
Surgeons and their patients benefit from the surgeon’s use of automated motor sequences. Automaticity allows the surgeon to execute complex motor sequences with relatively little cognitive load, freeing up cognitive space to attend to other aspects of surgical performance and optimal patient care. However, while beneficial, automated motor sequences may be difficult for skilled performers to describe or teach to others, to modify, or to break down into component parts (Hamdorf & Hall, 2000). In the case of veterinarians, much of this automation is likely to occur after formal surgical instruction has ceased. Thus, the grasp and movement patterns they ultimately adopt may be based on trial-and-error modifications to the techniques they were originally taught. The resulting variations in technique may be adaptive and beneficial, or they may be adequate but sub-optimal solutions in terms of biomechanics or performance (Bartlett et al., 2007).
In addition to diversity of grasps between surgeons, this study also noted instances of variability within individual surgeons’ grasps and movement patterns. In some cases, skilled performers show more variability than novices in the movements that they use to complete a task (Madeleine, 2010; Madeleine et al., 2008). This may be due to flexibility built into the automated motor sequence that they have acquired, or due to the acquisition of more than one automated motor sequence that can be used to complete the same task. For those with flexibility in their automated motor sequence, it is thought that this variability is made possible by the redundant degrees of freedom available in multi-joint movements (Srinivasan & Mathiassen, 2012). This flexibility allows the performer to adapt to perturbations and uncertainty while still completing the task (Bartlett et al., 2007).
Some skilled performers possess more than one automated movement sequence to perform the same task, and have developed these redundant motor sequences through deliberate practice and refinement (Ericsson, 2004). Among participants in the current study, three reported modifying their grasp after completing veterinary school. Two of these reported making these modifications consciously, and both sometimes use palm grasp and sometimes use 1,4 tripod grasp, selecting their grasp based on ease, comfort, and the appropriateness of the grasp to the specific suturing task.
It is likely that there is no single, unique movement pattern that optimizes performance (Bartlett et al., 2007). All of the veterinarians in the current study are experienced in high volume spay and neuter surgery, and each has performed thousands of procedures. The diversity in grasps, movement patterns, and muscle use described in this study all represent functional variations upon the task of suturing. Nonetheless, surgeons may benefit from developing multiple functional movement patterns that can be used to achieve the same task, both because this flexibility may lead to improved surgical performance, and because the increased variability may decrease repetitive strain.
Differences between individuals performing the same task make it difficult to characterize biomechanical exposure and consequent risk based on job description or work hours, and also suggest a possible mechanism for the differences between individuals in MSD susceptibility (Srinivasan & Mathiassen, 2012). The current study did not evaluate variability per se, and only examined a single task within the larger task of surgery, so was not adequate to see the scope of variability within spay neuter work. Future research could examine whether increased motor variability in surgery can be taught, and if so, the optimal amount and type of variability. Also, future studies could examine whether teaching a new grasp and motor sequence could allow a surgeon to recover from MSD, and whether surgeons with more than one grasp and corresponding automated motor sequence are more resilient than those with a single movement pattern.
Conclusions
The present study found an unexpected diversity of needle holder grasps used by spay neuter veterinarians while suturing. All were characterized by extensor dominance during static load. Future investigation into the characteristics and benefits of various grasps is warranted, so that practical advice on reducing strain and MSD risk can be offered to surgeons. In addition, examination of current surgical instruction and learning may help explain the origination of the diversity of grasps encountered here.
References
Adams, S.R., Hacker, M.R., McKinney, J.L., Elkadry, E.A., & Rosenblatt, P.L. (2013). Musculoskeletal pain in gynecologic surgeons. Journal of minimally invasive gynecology, 20(5), 656-660.
Anderson, R.M., & Romfh, R.F. (1980). Technique in the use of surgical tools. New York: Appleton-Century-Crofts.
Bartlett, R., Wheat, J., & Robins, M. (2007). Is movement variability important for sports biomechanists? Sports Biomech, 6(2), 224-243. doi: 10.1080/14763140701322994
Berguer, R., Gerber, S., Kilpatrick, G., Remler, M., & Beckley, D. (1999). A comparison of forearm and thumb muscle electromyographic responses to the use of laparoscopic instruments with either a finger grasp or a palm grasp. Ergonomics, 42(12), 1634-1645. doi: 10.1080/001401399184721
Booth, H.W. (2013). Instrument and tissue handling techniques. In K. M. Tobias & S. A. Johnston (Eds.), Veterinary surgery: Small animal: 2-volume set (pp. 201-213): Elsevier Health Sciences.
Criswell, E. (2011). Cram’s introduction to surface electromyography (2nd ed.). Sudbury, MA: Jones & Bartlett Publishers.
de Almeida, P.H., da Cruz, D.M., Magna, L.A., & Ferrigno, I.S. (2013). An electromyographic analysis of two handwriting grasp patterns. Journal of electromyography and kinesiology, 23(4), 838-843. doi: 10.1016/j.jelekin.2013.04.004
Ericsson, K.A. (2004). Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Academic Medicine, 79(10), S70-S81.
Esser, A.C., Koshy, J.G., & Randle, H.W. (2007). Ergonomics in office-based surgery: A survey-guided observational study. Dermatologic surgery, 33(11), 1304-1313; discussion 1313-1304. doi: 10.1111/j.1524-4725.2007.33281.x
Graybiel, A.M. (1998). The basal ganglia and chunking of action repertoires. Neurobiology of learning and memory, 70(1), 119-136.
Hägg, G., Melin, B., & Kadefors, R. (2004). Applications in ergonomics. In R. Merletti & P. Parker (Eds.), Electromyography: Physiology, engineering, and noninvasive applications (pp. 343-363). Hoboken, NJ: John Wiley & Sons, Inc.
Hamdorf, J., & Hall, J. (2000). Acquiring surgical skills. British Journal of Surgery, 87(1), 28-37.
Hedge, A. (n.d.). Cornell musculoskeletal discomfort questionnaires (cmdq). Retrieved 4 January, 2015, from http://ergo.human.cornell.edu/ahmsquest.html
Kirpensteijn, J., & Klein, W. (2006). Instruments. In J. Kirpensteijn (Ed.), Cutting edge: Basic operating skills for the veterinary surgeon (pp. 31-43). Ripon: Roman House Publishers Ltd.
Kozak, A., Schedlbauer, G., Peters, C., & Nienhaus, A. (2014). Self-reported musculoskeletal disorders of the distal upper extremities and the neck in german veterinarians: A cross-sectional study. PLoS ONE, 9(2), e89362. doi: 10.1371/journal.pone.0089362
Latko, W.A., Armstrong, T.J., Franzblau, A., Ulin, S.S., Werner, R.A., & Albers, J.W. (1999). Cross-sectional study of the relationship between repetitive work and the prevalence of upper limb musculoskeletal disorders. American Journal of Industrial Medicine, 36(2), 248-259. doi: 10.1002/(SICI)1097-0274(199908)36:2<248::AID-AJIM4>3.0.CO;2-Q
Looney, A.L., Bohling, M.W., Bushby, P.A., Howe, L.M., Griffin, B., Levy, J.K., Eddlestone, S.M., Weedon, J.R., Appel, L.D., Rigdon-Brestle, Y.K., Ferguson, N.J., Sweeney, D.J., Tyson, K.A., Voors, A.H., White, S.C., Wilford, C.L., Farrell, K.A., Jefferson, E.P., Moyer, M.R., Newbury, S.P., Saxton, M.A., Scarlett, J.M., Association of Shelter Veterinarians, S., & Neuter Task, F. (2008). The association of shelter veterinarians veterinary medical care guidelines for spay-neuter programs. Journal of the American Veterinary Medical Association, 233(1), 74-86. doi: 10.2460/javma.233.1.74
Madeleine, P. (2010). On functional motor adaptations: From the quantification of motor strategies to the prevention of musculoskeletal disorders in the neck-shoulder region. Acta physiologica, 199 Suppl 679, 1-46. doi: 10.1111/j.1748-1716.2010.02145.x
Madeleine, P., Voigt, M., & Mathiassen, S.E. (2008). The size of cycle-to-cycle variability in biomechanical exposure among butchers performing a standardised cutting task. Ergonomics, 51(7), 1078-1095. doi: 10.1080/00140130801958659
Matern, U., Kuttler, G., Giebmeyer, C., Waller, P., & Faist, M. (2004). Ergonomic aspects of five different types of laparoscopic instrument handles under dynamic conditions with respect to specific laparoscopic tasks: An electromyographic-based study. Surgical Endoscopy And Other Interventional Techniques, 18(8), 1231-1241.
McAtamney, L., & Corlett, E.N. (1993). Rula: A survey method for the investigation of work-related upper limb disorders. Applied Ergonomics, 24(2), 91-99.
Perotto, A. (2011). Anatomical guide for the electromyographer: The limbs and trunk: Charles C. Thomas Publisher, Limited.
Scuffham, A.M., Legg, S.J., Firth, E.C., & Stevenson, M.A. (2010). Prevalence and risk factors associated with musculoskeletal discomfort in new zealand veterinarians. Applied ergonomics, 41(3), 444-453. doi: 10.1016/j.apergo.2009.09.009
Seki, S. (1988). Suturing techniques of surgeons utilizing two different needle-holder grips. American journal of surgery, 155(2), 250-252.
Smith, D.R., Leggat, P.A., & Speare, R. (2009). Musculoskeletal disorders and psychosocial risk factors among veterinarians in queensland, australia. Australian veterinary journal, 87(7), 260-265. doi: 10.1111/j.1751-0813.2009.00435.x
Soueid, A., Oudit, D., Thiagarajah, S., & Laitung, G. (2010). The pain of surgery: Pain experienced by surgeons while operating. International journal of surgery, 8(2), 118-120. doi: 10.1016/j.ijsu.2009.11.008
Srinivasan, D., & Mathiassen, S.E. (2012). Motor variability in occupational health and performance. Clinical biomechanics, 27(10), 979-993. doi: 10.1016/j.clinbiomech.2012.08.007
Szeto, G.P., Straker, L.M., & O’Sullivan, P.B. (2009). Examining the low, high and range measures of muscle activity amplitudes in symptomatic and asymptomatic computer users performing typing and mousing tasks. European journal of applied physiology, 106(2), 243-251. doi: 10.1007/s00421-009-1019-4
Toombs, J.P., & Bauer, M.S. (1993). Basic operative techniques. In D. Slatter (Ed.), Textbook of small animal surgery (2nd ed., Vol. 1, pp. 168-191). Philadelphia, PA: Saunders.
Weiss, Y. (1973). Simplified method of needle-holder handling. Archives of Surgery, 106(5), 735-736.
White, S. (2013). Prevalence and risk factors associated with musculoskeletal discomfort in spay and neuter veterinarians. Animals, 3(1), 85-108.
Yoon, H.-Y., & Mann, F.A. (2011). Instrument handling. In F. A. Mann, G. M. Constantinescu & H.-Y. Yoon (Eds.), Fundamentals of small animal surgery (pp. 128-142).
As a rule, the needle should be grasped at its center or perhaps 50-60% back from the pointed end. The needle should be grasped 1-2 mm from the tip of the needle holder.