
After writing this blog for a few years now, I realized that I haven’t explained what I do for my “day job” as an HQHVSN veterinarian. I am the Executive Director and Veterinarian at Spay ASAP Inc., a MASH-style spay neuter clinic in Vermont and New Hampshire.
(Parts of the content for this post are adapted from Chapter 34 of the textbook, High Quality High Volume Spay Neuter and Other Shelter Surgeries)
What is a MASH clinic?
MASH (Mobile Animal Sterilization Hospital) clinics are a type of mobile spay-neuter program in which clinic staff transport surgical equipment to a venue and set up a temporary surgical space in that location. Surgeries are not performed in the MASH vehicle, but instead utilize an existing space in the community.

Examples of clinic locations that I’ve used include animal shelter buildings, church basements, animal care (grooming and boarding) facilities, fire stations, town offices, school gymnasia, senior centers, and many more.

MASH programs vary in the number of surgeons, technicians, and support staff, the frequency of surgery days, the number of consecutive days at a single venue, and in mission and organizational structure. Some MASH programs work independently of other humane organizations (independent MASH programs), while others conduct all their work in collaboration with other humane organizations (collaborative MASH programs). Over the years, Spay ASAP has been hosted by over 15 different humane organizations in Vermont and New Hampshire, and currently we are hosted by 8 different organizations and also have a few additional humane organizations that bring animals to our clinics.
Venues

Venues for MASH clinics may be diverse and creative, but with few exceptions, MASH clinics require an enclosed space of a minimum of 1000 square feet (preferred 2000 square feet or greater) that can be maintained at a safe, comfortable temperature, and access to hot and cold water and electricity. In cases where running water is not available, hot and cold water may be brought to the venue. Facilities may be able to provide large nonmedical objects such as folding tables, chairs, and trash receptacles; if not, these items should be provided by the host organization.
Animal Housing

Since many MASH clinics do not take place in animal care facilities, animal housing often consists of pet carriers or folding wire cages. In these cases, host groups should be prepared to provide crates and bedding for housing dogs, as many owners will not have or will not be able to transport appropriate crates or cages for their dog. Cats and rabbits are generally housed in the carriers in which they arrive at the clinic, and community cats remain in their traps. It is wise to have additional crates available in which to house cats who arrive in inappropriate or inadequate housing.


MASH Equipment
Equipment requirements for a MASH clinic are similar to those in other clinic types, but all items must be compact and packable, and must have the durability to withstand transport, packing and unpacking daily. Choices for surgery table, surgery light, and anesthesia machines will be influenced by this need for packability and durability.
Vehicle

For our MASH vehicle, we needed space for 2 people and the necessary equipment. A small minivan, a compact SUV, a station wagon, or a boxy passenger car are adequate for a collaborative MASH program. Small, mass-market vehicles have the advantage of low purchase price, good fuel economy, and low maintenance costs.

Anesthesia Equipment

Like many MASH clinics, we use inhalational agents (isoflurane) for some of our patients’anesthesia. We have two anesthesia machines: one for the surgical prep area and one for surgery. This allows animals in the prep area to receive oxygen and anesthetic gas while they are being clipped and scrubbed, so that when they arrive on the surgery table they are on a steady anesthetic plane for surgery.

Tabletop anesthesia machines are easy to carry and need not be disassembled to pack in a small vehicle. Our current machines were custom made by Eagle Eye Anesthesia. We use a Tec 4 type vaporizer (the big, square-bottomed heavy ones) since they contain internal baffles that limit the movement of the anesthetic agent. Basically, they continue to deliver appropriate anesthetic concentrations even if the vaporizer is temporarily tipped or upended (ie, when the machine falls out upside down onto the ground when you open the car door).

For oxygen we use portable E cylinders in 2-wheeled oxygen cylinder carts and attached to the anesthesia machine via a regulator and oxygen hose. Oxygen cylinders should be immobilized in the vehicle for transport.
For anesthetic gas scavenging, we usually use passive scavenging (unless we are in a venue with a surgical suite with active scavenging). Passive scavenging options include exhaust through a window, through a hole made in the wall, or using an activated charcoal absorbent canister such as a F/Air canister.



Equipment Bins
Small equipment and supply items used during the MASH surgery day are packed in bins or totes for organization and ease of transport . We sort our bins by type of items: needles and syringes in one bin, anesthesia tubing and bags in another. We have smaller bins for surgery packs that hold about a dozen packs each.



A rolling cart is also helpful for venues with level entrances, allowing us to make fewer trips between the car and the surgery area during setup and takedown.
Surgery Table and Light

Some MASH programs require that host organizations provide appropriate height surgery and prep tables and a surgery light at each venue. This is most easily achievable if clinic venues are used repeatedly and are owned by the host organization. In these cases, steel food service tables or appropriate-height tables constructed by volunteers offer alternatives to commercial surgery tables.
At Spay ASAP, we went with a different option and have a portable surgery tabletop, allowing for greater flexibility in temporary surgery venues. A portable tabletop may be constructed using a piece of countertop with folding legs at a fixed or adjustable height that can be placed atop a standard height table– ours was made from a piece of countertop that once went over a dishwasher. We use a small bin (a surgical instrument bin) as an instrument stand.

Other portable table alternatives would include using a small or standard folding table with bed risers or an adjustable-height folding table. We also elevate the surgical prep table to the appropriate height for the veterinary technician using bed risers or blocks.
For surgical lighting, we use an architect’s lamp with a compact fluorescent bulb of 23 watts or greater, or LED bulb of 16 watts or greater (equivalent to a 100-watt incandescent bulb). Alternatively, a head lamp may be used, but I find the weight of these lamps to be uncomfortable and am less impressed by the lighting quality.
Patient warming
Selecting a surgical patient warming device for MASH can be challenging, as some are too bulky to transport in small MASH vehicles, and those containing water may be difficult to transport due to spilling or freezing water during transport and storage (I used to use a Gaymar pump and water blanket but got frustrated by leaks and spills and the risk of freezing). A low-voltage conductive polymer fabric heating pad (such as Hot Dog or ChillBuster or Warm Blood if you can still find them) can be used, as they are compact and fairly durable.
Any postoperative warming devices that we use, such as heating pads, rice socks, or electric blankets, are supplied by the host organization, and should be used with caution (ie, no skin contact with the pet, and used only with direct human supervision) to avoid thermal burns.
Additional Equipment

Additional equipment transported by the MASH clinic includes a scale to weigh surgery patients, anesthesia monitor(s) such as a pulse oximeter or capnograph, anti-fatigue floor mats, and an insulated container for vaccines.
Safety equipment such as cat net, animal handling gloves, syringe pole, squeeze cage, and dog muzzles should be included, as many venues will not have adequate handling equipment. An additional useful piece of handling equipment is a snappy snare, which is a 3- to 5-foot-long stiff leash that allows the leash to be placed on the dog from a distance, and is useful for safely applying a leash to a frightened dog in a crate or kennel.
“Home Base”

MASH clinics require a small area (minimum 10 x 10 feet) for receiving and storage of supplies and medications. At Spay ASAP, we rent a room on the second floor above a veterinary hospital. The ideal space would be easy to access with a convenient geographic location, a convenient physical location (first floor, near supply delivery area), and is temperature controlled for safe medication storage. Our space isn’t ideal from the point of view of deliveries, but we do have direct access via the fire escape.
If the MASH program is part of existing organization with a physical building, the MASH clinic can use this space.
If the MASH is a new organization or has no suitable site, possible sites include the home of a staff member or a rental space. Renting space from an existing animal care organization such as a veterinary clinic offers the advantage of on-site staff to receive deliveries of temperature-sensitive items such as vaccines or medications.

If the home base is to be used for surgical pack preparation, it should contain or allow access to laundry facilities (unless all drapes and pack wrappers are disposable) and electricity, and should be large enough to accommodate pack assembly and an autoclave. During times when we have prepared packs in our rental space, we have rented additional space in order to have table space to prepare packs.
How to set up a MASH program: organizational structure and details
Everything from here on is more nitty gritty organizational detail, including more words, no pictures, and more generalizable information. It draws heavily from the MASH textbook chapter. It may be a bit too detailed for a blog post, but I wanted to get this information out and available for anyone who is really interested in starting up this type of clinic.
Can I MASH here? Legal issues:
Before considering a MASH clinic, be certain to check any relevant state or provincial veterinary practice acts and local regulations to be sure that MASH clinics are permitted. Some states and provinces require premise permits for any practice location, which may preclude MASH clinics. However, in some cases, states or provinces that require premise permits may allow exemptions for MASH clinics if asked in advance.
Who should MASH?
MASH clinics are adaptable and there are not specific prerequisites for regional population density or shelter animal intake. They are suitable for rural areas where low population density does not easily support a stationary clinic (like the border area of Vermont and New Hampshire), as well as for densely populated urban areas. MASH clinics are valuable for local shelters that wish to provide in-house HQHVSN, but either cannot afford to build and equip their own surgical suites, or that have surgical areas but lack veterinary staff. MASH clinics are also suitable for international and remote area spay-neuter programs.
For a veterinarian with surgery skills seeking spay-neuter work, establishing a MASH clinic can be one of the fastest and lowest cost ways of starting a HQHVSN clinic. This is what I did when I started Spay ASAP in 2006, and we went from registering the nonprofit in March to performing our first surgery in early June. In most cases, veterinarians who choose this route should be willing to operate the business aspects of the clinic and be able and willing to work with shelters and humane organizations in their target region.
In some cases, programs with limited startup funds may wish to offer surgery services before fundraising is complete or before a clinic site is located for a future stationary clinic. In this case, a MASH clinic may serve as a temporary economical option during the development of the HQHVSN program. Since any equipment purchased for MASH can be used in other models, the MASH clinic provides the opportunity for quicker startup without loss of equipment investment.While MASH programs are diverse, this chapter will focus on programs that utilize paid veterinarian(s) and technician(s) and operate within a prescribed region (as opposed to national or international scope). However, many of the descriptions in this chapter may be adapted to MASH programs that operate internationally and/or use volunteer veterinarians and technicians. For information on setting up international or remote area MASH clinics, the reader is referred to Susan Monger’s chapter on Operating a field Spay Neuter Clinic in the Field Manual for Small Animal Medicine.
Independent versus Collaborative MASH programs
MASH programs can operate their clinics independently of other humane organizations in a region or may collaborate with other humane or community organizations to host their clinics. Some MASH clinics may use a combination of these two approaches. There are advantages and disadvantages to each of these models. My own Spay ASAP clinics are collaborative MASH clinics so I’m biased towards that model and find it to be sustainable over the long term.
Collaborative MASH programs
Collaborative MASH programs are generally small organizations that collaborate with various local humane or community groups that act as their hosts in the communities within their service area. These host groups (or “ground teams”) must provide the venue and personnel, consisting of 2-5 staff members or volunteers, while the MASH program (or “surgery team”) provides the veterinarian, the technician, and all surgical supplies and equipment. The host organization is responsible for scheduling, admitting, and discharging patients, and for printing, preparing, and distributing clinic paperwork such as medical record forms, liability releases, discharge instructions, rabies certificates, and neuter certificates. Host groups are often required to provide non-medical supplies such as tables, chairs, animal bedding, extra pet carriers, and trash receptacles. In these collaborative programs, the MASH group generally works with several different host organizations throughout their service area to host clinic days. At times, more than one local humane group may work together to host a MASH clinic.
Collaborative MASH programs empower small humane organizations and shelters to host their own “Spay Days,” affording them the opportunity to enhance their community relations and outreach. The opportunity to host and assist with a MASH clinic enables staff and volunteers at host shelters to do something “fun” and different, compared to their usual shelter duties. These collaborations also allow opportunities for MASH clinic staff to share information and best practices for shelter medicine and HQHVSN with their host organizations.
Generally, it is the responsibility of the MASH organization to provide training and mentorship to new or potential new host organizations. Before hosting their first clinic, host organizations will need to know how to schedule the appropriate surgical load and how to determine the number and skill level of volunteers required. They need to understand the paperwork and be able to provide appropriate pre- and post-operative instructions to clients. An in-person meeting between the MASH organization and potential new hosts along with written instructions on hosting protocols and expectations is recommended prior to the first clinic.
Once a MASH organization has established relationships and carried out clinics with one or more host organizations, potential new host organizations can benefit greatly by visiting with and observing existing host organizations during MASH clinic days. This peer-to-peer mentorship helps new host organizations develop their own protocols and systems and allows them to see clinic flow and ask questions before their first clinic. In some cases, this mentorship may even continue, with representatives from existing host organizations attending the first few clinics sponsored by new host organizations, smoothing their transition into their role as host.
Advantages of the collaborative MASH model include flexibility and decreased operating costs. Staffing costs are decreased for the MASH organization because of the symbiotic relationship between the MASH organization and their hosts. The MASH organization pays only one veterinarian and one technician per day, in addition to an after-hours surgical pack preparation staff, and relies upon the host organization to provide additional resources (2-5 staff or volunteers, and venue). The hosts are motivated to provide this because they need the MASH program’s staff, equipment, and expertise in order to offer affordable HQHVSN clinics.
In contrast to an independent MASH clinic, the collaborative MASH clinic requires a relatively small vehicle given the small staff and minimal equipment required. Purchasing a smaller vehicle results in a lower initial purchase price, as well as lower ongoing fuel and maintenance costs. This decreased operating cost often means that a collaborative MASH clinic is able meet their budget entirely via low-cost fees for service, without additional fundraising.
Independent MASH programs
Independent MASH programs have sole responsibility for scheduling the venue, booking patients, securing volunteers and staff, and admitting and discharging patients. The independent MASH model is more likely to be adopted by large, pre-existing organizations, by new HQHVSN programs planning to transition to stationary clinics in the future, or by organizations doing MASH clinics intermittently. This is because developing and training the network of collaborating host organizations that is required for a collaborative MASH clinic takes time and effort. For large, established organizations that have the resources to perform ground team tasks in addition to surgical team tasks, this extra task of collaborator development may be unnecessary. For MASH clinics that operate intermittently, the collaborative relationships may languish and be harder to maintain.
In an independent MASH clinic, staffing and finances are likely to be similar to a stationary clinic or self-contained mobile surgery unit, unless adequate, reliable volunteer staffing is available. Minimal required staff would consist of a veterinarian, a veterinary technician, one or more veterinary assistants, and administrative staff for record keeping, patient booking and reception.
Independent MASH clinics may require larger vehicles than collaborative programs to transport staff, surgical equipment, and some nonmedical items such as animal bedding and extra pet carriers or crates. Since the staffing for this model of clinic is similar to that of a stationary clinic, the costs are higher as well, making this model harder to sustain financially than collaborative MASH clinics. However, independence can offer the advantage of more predictability by utilizing more consistent clinic staff and by not needing to rely on other humane groups to schedule clinic dates and locate suitable staff and volunteers.
Organizational structure
MASH clinics may be established within any organizational structure, including nonprofit, for profit, and government or tribal entities. In some cases, MASH clinics may represent a single program within a large, diverse existing organization. For example, an animal shelter with an in-house spay-neuter clinic may develop a MASH program to reach certain communities in their service area. In others, a new organization is formed for the purpose of offering MASH clinics, and this organization exists solely for the purpose of offering MASH clinics.
Financial investments and ongoing costs
Financial requirements for a MASH clinic are generally much lower than for a stationary clinic or self-contained mobile unit. There will also be some differences in the initial investments between MASH clinics following a collaborative model versus an independent model. In all MASH clinics, the major initial costs will include acquisition of a vehicle, surgical and anesthetic equipment, initial consumable supplies (for example, drugs, vaccines, syringes and needles, gauze sponges, antiseptics, and suture material) and an autoclave. In cases in which the MASH clinic already has access to a suitable vehicle, or if the MASH vehicle is purchased with a car loan, the initial investment to start a collaborative MASH clinic will likely range from $20,000- $35,000.
Ongoing costs for MASH will include personnel costs (salaries, wages, benefits, payroll taxes, workers compensation), consumable supplies, and vehicle gas and maintenance. Most MASH clinics will also need to rent a small, climate-controlled “home base” physical space for safe storage of consumable supplies (see “home base” section above).
Because overhead costs are low, it is possible to sustain a collaborative MASH clinic with low-cost fees for services, without additional fundraising. In cases where extremely discounted or free surgeries are to be offered, additional fundraising and grant writing by the MASH clinic or by one or more host organizations will be required to subsidize program costs.
Personnel
Minimal personnel requirements for a collaborative MASH clinic generally consist of one veterinarian and one veterinary technician. Some MASH programs employ additional staff for instrument care or for management. In many collaborative MASH programs, the veterinarian and technician handle instrument care and management responsibilities without additional staff. For example, the veterinarian serves as the program director/manager, and the technician assumes the responsibility for preparing surgical packs.
Independent MASH programs require additional personnel including veterinary assistants and administrative staff. The staffing model for these clinics is similar to that for a stationary or mobile self-contained clinic.
Surgical capacity
Surgical capacity for a MASH clinic should be comparable to other HQHVSN models, although in many MASH clinics, only one surgery table is available, so surgical flow and resulting speed is somewhat slower than in a fully-equipped stationary clinic. However, unlike in some self-contained mobile units, physical space for animal housing need not be a limitation for MASH clinics. Approximately 5 hours of surgery time is a full day for a MASH clinic, and this may consist of as few as 15-20 dogs or as many as 50-60 cats for one veterinarian depending on surgical speed and species and sex composition of the patient load.
Timeline
Startup time for a MASH program can vary. In the case of collaborative MASH programs, startup may be delayed if collaborating organizations need to be identified and persuaded. However, if collaborating organizations are prepared to host clinics immediately, a MASH program can start up in less than 3 months once finances are obtained.
Protocols
As with all HQHVSN clinics, MASH clinics should adhere to the ASV Guidelines for Spay-Neuter Programs. Surgery techniques, patient selection, and disinfection and sterilization of equipment are no different than in other HQHVSN clinics. Anesthesia and analgesia protocols are similar to those in stationary clinics, although care must be taken to select protocols that are suitable for same-day discharge of patients. As with all clinic types, proper medical record-keeping is essential, and clients must be provided with written and verbal postoperative instructions.
Post-operative care
As with other clinic types, there is a need to develop a postoperative care plan for emergencies and client questions. In most cases, this is achieved by providing a phone number to clients to contact MASH clinic staff in case of questions or emergencies. This phone may be carried by a veterinarian or a technician who can answer client questions and concerns and triage cases requiring veterinary care. For independent MASH clinics, administrative staff may carry this phone, triage calls, and refer medical questions to a veterinarian. Emergencies and rechecks will generally need to be seen by outside veterinary hospitals, as the MASH staff may be distant from the animal in question and may have no available facility in which to see patient rechecks. It is up to the MASH program to set policies with regards to client reimbursement or payment to outside veterinary hospitals seeing MASH clients. In many MASH clinics, as with other HQHVSN clinics, outside care is reimbursed if related to the surgical or anesthetic procedure, and if the client has generally followed post-operative instructions.
Some MASH programs have established relationships with specific local veterinarians or emergency clinics within their service areas who are willing to provide emergency care, and in some cases, the clients may be provided with this contact information instead of or in addition to contact information for the MASH clinic. Other MASH programs establish relationships with local practices as needed, as the geographical areas covered by some MASH programs are large enough that specific local relationships may be difficult to establish. Regardless, it is essential that the MASH clinic have a plan in place for how they will address follow-up or emergency care for their patients.
Surgical Instruments and their Care
In most cases, MASH clinics have no on-site autoclave. Most surgical instrument care, including ultrasonic cleaning, pack preparation and autoclaving, takes place after hours or between clinic dates. Thus, many small, collaborative MASH clinics maintain enough sterile surgical packs for multiple (2-3) days-worth of surgery or schedule time in between surgery days to provide time for packing and sterilization. This may be especially important if the pack preparation is performed by staff who are also members of the traveling MASH clinic team.
Surgical instruments should be soaked to remove organic debris and cleaned by hand by volunteers at the surgical venue, then rinsed and returned to the transport vehicle to be transported back to the home base with the surgical team. Further instrument cleaning, laundering of drapes and pack wrappers, pack preparation, and sterilization may occur at the MASH clinic’s home base, or alternatively may take place in a staff member’s home. This at-home pack preparation and autoclaving may be advantageous if the staff member lives far from the home base, or if the staff member has household obligations (such as small children) that make after-hours travel to the home base difficult.
MASH: The Day of Surgery
MASH clinics are typically located in different venues with a different layout each day. Collaborative MASH clinics work with different assistant staff each day, as provided by the host organization. These changes can affect clinic flow and efficiency, and they require the MASH veterinarian and technician to adapt to a variety of new situations and circumstances.
Setting up the clinic
In a collaborative MASH clinic, the host organization’s staff admits patients before the veterinarian and technician arrive, or while the veterinarian and technician are unpacking and setting up. In each new clinic venue, the MASH veterinarian and technician must plan the layout and flow for the clinic. The veterinarian’s and technician’s workspaces are re-created as consistently as possible but must be adjusted to accommodate the locations of windows, electrical outlets, and doors. Flow through the clinic should be optimized, although not every venue will lend itself to smooth flow between preop, prep, surgery, recovery, and postop areas.
Clinic Flow
Clinic flow in a MASH program may be somewhat slower than flow in a stationary clinic. Typically, a MASH clinic has one surgery table per surgeon, such that the surgeon must wait while patients are exchanged on the table. To improve flow while working on cats, the surgeon may alternate male and female cats, castrating male cats on a side-table or countertop while female cats are exchanged on the surgery table. MASH clinics also usually have only one prep station, which may be the rate-limiting step during fast surgeries. Also, since clinic layout and staffing vary between locations, ideal flow may not be achievable at each clinic site.
Clinic Day
The MASH clinic day includes travel, setup, and re-packing, in addition to the usual tasks related to operating a HQHVSN clinic such as performing patient exams, anesthetic procedures, and surgery. The total day length for the veterinarian and technician may be 11 hours, whereas the surgery time is only 4-5 hours. Thus, more than half the staff’s time is spent driving, setting up, and re-packing the surgery area. This time budget may be improved somewhat by changing clinic policies: driving time may be reduced by restricting the travel radius, and setup and takedown time may be reduced if the clinic is located in the same venue for multiple days.
The time required for these additional tasks of driving, setup, and packing means that MASH clinics are not the most efficient clinic model in regards to use of the veterinarian’s and technician’s professional time. A MASH that employs only one veterinarian and one technician may be operating “full time” (36-40 hours a week) with just 3 clinics—or about 100 surgeries—per week, if the technician is also preparing packs between surgery days, and the veterinarian is acting as administrator and business manager. However, despite achieving fewer surgeries per full-time veterinarian, the lower overhead costs mean that the cost-per-surgery is equivalent to that of a stationary clinic. This allows MASH clinics to pay hourly wages to the veterinarian and technician that are on a par with, or in some cases greater than, stationary or self-contained mobile HQHVSN clinics.
MASH clinics provide a flexible, low-cost, high-quality method for delivering spay-neuter services. The MASH clinic’s versatility, adaptability, relatively low capital investment, and short time to start up are the particular strengths of this clinic type, and makes these clinics useful both as short-term solutions as well as long-term, sustainable HQHVSN providers.
I hope you all enjoyed this intro to MASH clinics!




















 It may not be possible to avoid extreme neck flexion in this work, and the important thing will be getting out of this posture between surgeries to allow those muscles to release and stretch. Turning your neck to each side, rolling your head, extending your neck, and shrugging your shoulders are all ways to release the tension in the muscles around your neck.
It may not be possible to avoid extreme neck flexion in this work, and the important thing will be getting out of this posture between surgeries to allow those muscles to release and stretch. Turning your neck to each side, rolling your head, extending your neck, and shrugging your shoulders are all ways to release the tension in the muscles around your neck. However, varying position during the surgery day is a good thing. If this surgeon balances the twist in one direction over time with a twist in the other direction, then she may not experience strain from the posture.
However, varying position during the surgery day is a good thing. If this surgeon balances the twist in one direction over time with a twist in the other direction, then she may not experience strain from the posture.





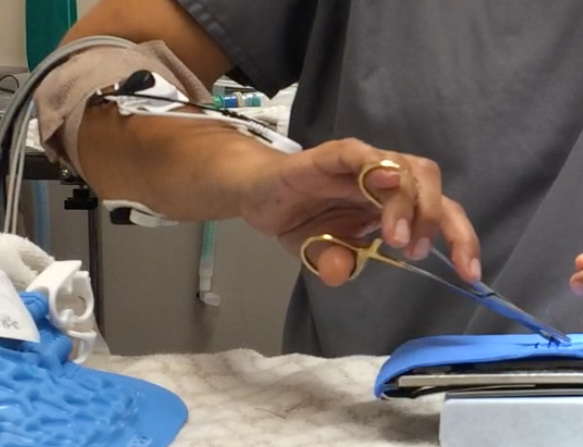
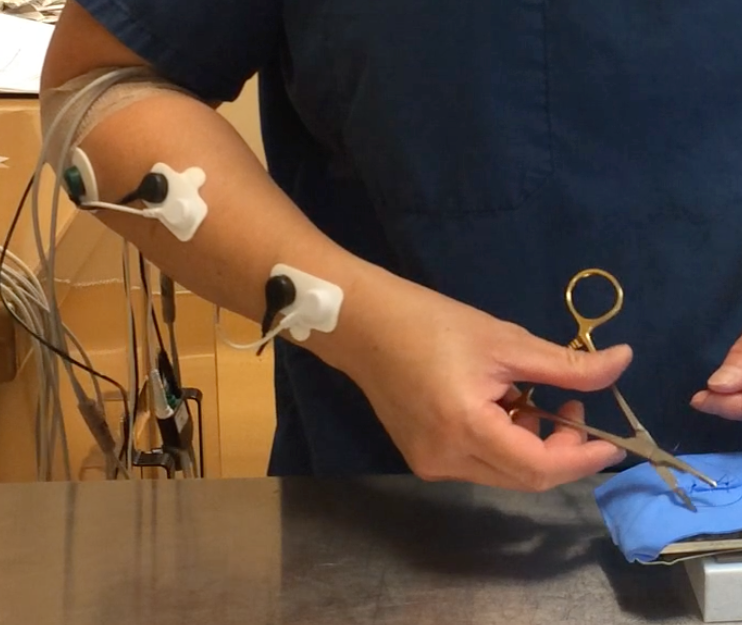
 (These vets have wires and stick-on electrodes on their arms because they were a part of my Masters’ research project).
(These vets have wires and stick-on electrodes on their arms because they were a part of my Masters’ research project).



 The moral is, if you’re doing something really awkward, there is probably another solution that is a lot smoother and easier.
The moral is, if you’re doing something really awkward, there is probably another solution that is a lot smoother and easier. Choosing a suture size that is bigger than what you need for a given surgery means that on every throw of every knot, you will be applying more pounds of force to your ligaments and muscles. Over the course of a surgery day, that’s hundreds of times that you’re applying that extra force.
Choosing a suture size that is bigger than what you need for a given surgery means that on every throw of every knot, you will be applying more pounds of force to your ligaments and muscles. Over the course of a surgery day, that’s hundreds of times that you’re applying that extra force. Some alternatives that decrease this strain could include
Some alternatives that decrease this strain could include










